Diffuse Hair Loss: Causes and Treatment
By Dr. Rashmi Singh, MD – Updated on November 25, 2020

Scalp hair is like salt in your food; if you have it in an appropriate quantity, you don’t realize its importance, but lacking it suddenly becomes an essential ingredient of the dish. Since hair loss causes are diverse, treatment or approach is ineffective if the cause is not identified.
This article will discuss the common and not-so-common causes of diffuse hair loss in males and females and a standard approach to hair loss.
Causes of diffuse hair loss
Diffuse hair loss means thinning hair from a large surface of the scalp, which can sometimes involve the entire scalp. The common causes of diffuse hair loss involve a disruption in the hair cycle. Each hair follicle undergoes 10-30 cycles in its lifetime.
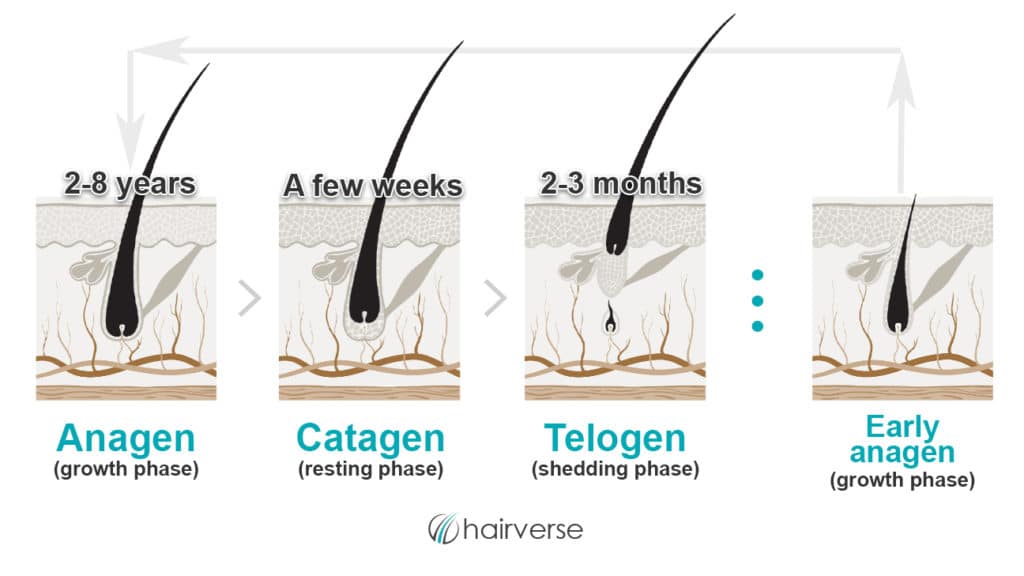
Each hair follicle has an independent cycle, but since, at any point in time, multiple hairs are in the same phase, the total number of hairs remains constant.
At any given time, an estimated 75-80% of hairs are in the anagen, 10-15% in catagen und another 10-15% in the telogen phase. A shedding of up to 100 hairs in a day is considered normal.
The causes of diffuse hair loss can be classified broadly under:
1. Androgenetic alopecia
Commonly known as male or female pattern hair loss, androgenetic alopecia is often genetic and somehow starts showing first signs at a younger age with every successive generation and presents a big cosmetic issue.
People suffering from androgenetic alopecia do not complain of acute hair loss but a gradual thinning of hair over the years. It results from a reduction in the hair cycle duration successively and causes miniaturization of hair follicles.
These changes are due to the interaction between androgens (DHT) and its receptors in hair follicles.
It results from a progressive reduction of successive hair cycle time, leading to miniaturization of hair follicles. These changes are mediated through interaction between androgens, their respective receptors.
Female pattern hair loss is often pretty diffuse. The first signs of thinning are observed either over the crown, causing a widening of the central parting line, or along the frontal hairline. Male pattern hair loss almost always presents with a receding hairline and thinning over the vertex.
2. Acute telogen effluvium
Acute telogen effluvium is characterized by abrupt onset and diffuse shedding of hair, usually 2-3 months after a triggering event like an acute illness, trauma, crash diet, pregnancy, etc. and it involves the entire scalp.
At any point, around 10% of hair is in the shedding phase (telogen phase), and approximately 100 hairs lost daily is considered normal.
In an acute, distressing event, multiple hairs in the growing phase of the hair cycle (anagen) go abruptly into the telogen phase, causing a sharp increase in hair fall. It is usually self-limiting, and the excessive hair shedding stops in around 4-6 months.
A variation of telogen effluvium is called anagen effluvium, which occurs 1-3 weeks after initiation of chemotherapy where the hair, instead of going to the telogen phase, stays in anagen and starts falling.
3. Chronic telogen effluvium
Telogen effluvium persisting beyond six months is called chronic telogen effluvium. It happens when the cause of telogen effluvium is not identified and consequently not treated.
Two of the most common causes of chronic telogen effluvium are psychological stress and deficiency of iron reserves in the body (reduced ferritin levels). Other causes may include- medicine intake, hormonal imbalance, thyroid disorders, deficiency of vitamins/minerals- most commonly vitamin D and Zinc, etc. [1]
It presents with long-term (more than six months) more-than-normal hair shedding and can have a fluctuating course.
4. Alopecia areata totalis
Alopecia areata totalis is an autoimmune condition leading to loss of all the hair in the affected area (most commonly on the scalp, but can also involve other body parts), causing a bald patch.
It can be limited to hair loss from one or two patches on the scalp but may also involve the entire scalp. The progression of alopecia areata can be alarmingly fast. Even though it can sometimes be self-limiting when the whole scalp is affected, medical treatment is highly recommended.
5. Skin and scalp diseases
Many inflammatory diseases of the scalp can cause diffuse hair fall like lichen planopilaris, folliculitis decalvans, psoriasis, etc. The hair fall in such cases can either be reversible when the causative disease is treated or can destroy the hair follicles and make the hair loss permanent.
Thus, early medical intervention is indicated. If the hair loss is associated with redness, itching, or pain – a dermatologist should be consulted without delay.
6. Hair breakage
It is not technically ‘hair loss,’ but diffuse hair breakage could cause thinning hair and similar distress like actual hair fall. The most common causes of hair breakage are weathering hair through chemical and heat treatment, making the hair shaft very fragile and prone to breakage.
Treatment of diffuse hair loss
Treatment of diffuse hair loss first and foremost needs an accurate diagnosis. While androgenetic alopecia or alopecia areata can be diagnosed clinically just with the pattern of hair loss, other causes need a thorough history and investigations.
It is not rare to get overlapping telogen effluvium and androgenetic alopecia, or androgenetic alopecia and inflammatory skin diseases. Effective treatment includes the following:
1. General measures
– Diagnosis: Investigations, like an examination of the scalp, a hair pull test, a complete, exhaustive blood workup, a trichogram to roughly know anagen vs. telogen hair present in the scalp, and, if needed, a biopsy can give valuable information to make the correct diagnosis and start an effective treatment. [2]
It is also important to differentiate hair fall from hair breakage. In the case of hair breakage, nutrition deficiency should be ruled out, and intense repair measures should be undertaken.
– Dietary changes: A well-balanced diet and supplementation of deficient nutrients (like Zinc, Vitamin D, or Vitamin b12) could be instrumental in stabilizing hair fall. Anyone suffering from hair loss should have a calorie intake of more than 1200 kcal/day and a protein intake of 0.8g/kg body weight.
Contrary to popular opinion, biotin intake is not very helpful in hair loss unless you are biotin deficient, and biotin deficiency is extremely rare. So biotin supplementation could actually be fruitless, and thus, indiscriminate use of biotin should be avoided.
– Change in hair grooming habits: For all hair loss causes, gentle grooming of hair is advised. Very tight ponytails, extreme heat treatments, repeated combing, etc., can result in an increase in hair loss.
– Education: To avoid stress and disappointments, in all cases of diffuse hair loss, proper counseling with a physician is really instrumental. The normal course of the condition, overlapping factors, expectations from treatment should always be known to the patient. Not managing the causative stress related to hair fall can result in a vicious cycle by causing increased hair fall.
– Hair cosmetics: Even though shampoos, conditioners, or hair oils do not play a significant role in hair fall, selecting the wrong hair cosmetics can increase hair fall due to breakage. Mild but appropriate to hair type hair products always optimize the outcome of hair fall treatment.
– Regular follow-up with the treating physician: The plethora of information floating around on the internet increases the tendency towards self-diagnosis and self-treatment.
While it is not wrong to have a provisional diagnosis and treatment option based on your research, visiting a physician to confirm the diagnosis, explore the various treatment options, and evaluate the success of the treatments you have been doing improve compliance and results in diffuse hair loss.
2. Specific measures according to cause
– Androgenetic alopecia: First-line therapy to all patients of androgenetic alopecia, unless there are contraindications, involves minoxidil 2-5% to make the anagen phase longer and reverse the hair follicle miniaturization. If the patients respond to minoxidil, an improvement of hair loss is seen in around 3-6 months.
Suppose minoxidil alone does not give satisfactory results or is not tolerated. In that case, a systemic therapy like finasteride or anti-androgens can be added, which acts on DHT (dihydrotestosterone) and its receptors.
Starting a systemic treatment should be made only by a physician taking age, sex, side effects, and contraindication into consideration. Procedures like platelet-rich plasma and micro-needling can further support the treatment.
Since the hair fall in androgenetic alopecia is a continuous process, the treatment should also be continued indefinitely. The benefit of any form of treatment lasts only till it is used.
– Acute telogen Effluvium: If triggered by an acute and short-lived event like trauma or disease, acute telogen effluvium is self-limiting.
Hair stops shedding in around 3-4 months, and since it does not result in scarring, a complete regrowth is expected. If the trigger is continuous, like drug intake or crash diet, this needs to be addressed and corrected.
Topical solutions containing caffeine or peptide-based serums may have some help, but strong evidence is lacking. [3, 4]
Minoxidil and other procedural treatments should be avoided in the case of acute telogen effluvium.
– Chronic telogen effluvium: Chronic telogen effluvium needs a detailed workup to determine the cause, and that could be treated as a priority. Concomitantly, minoxidil 2-5% and peptide-containing topical preparations could help reduce hair loss.
Nutritional supplementation with amino acids, zinc, iron, copper, and folic acid support the treatment of chronic telogen effluvium. Platelet-rich plasma therapy, although not very effective, can stimulate new hair growth in stable chronic telogen effluvium.
– Alopecia areata totalis and inflammatory scalp diseases: While some inflammatory diseases of the scalp can be controlled by shampoos and topical medications like steroid lotions, alopecia totalis, and scarring alopecia could need systemic immunosuppressive treatment.
Since scarring alopecias are irreversible, urgent medical attention and early treatment are very important.
– Hair breakage: Hair breakage should be treated with deep conditioning treatments, avoidance of more damage, a complete break from chemical and heat treatments, and in case of nutritional deficiencies- with a proper balanced diet and supplementation.
Conclusion
Diffuse hair loss is a psychologically distressing condition, and the need for a proper diagnosis and treatment cannot be stressed enough.
Since there are so many causes, overlapping presentations, and diverse treatment options, it is advisable to seek a medical opinion to understand your hair loss, find the reason, and treat it most effectively.

